
EMS was called to the home of a 24-year-old female who was altered. She started acting “bizarre” and eventually became unresponsive, so her family called 911. The ambulance arrived and, per protocol for an altered level of consciousness patient, checked her blood sugar which they found to be 30. The patient was given IV dextrose D50 and immediately woke up.
The first thing she said when she woke up was, “I have chest pain.” An EKG was obtained. Her EKG showed normal sinus rhythm, no ectopy, and normal axis but a large Q wave in lead III. The EKG read also said, “possible old inferior MI.”
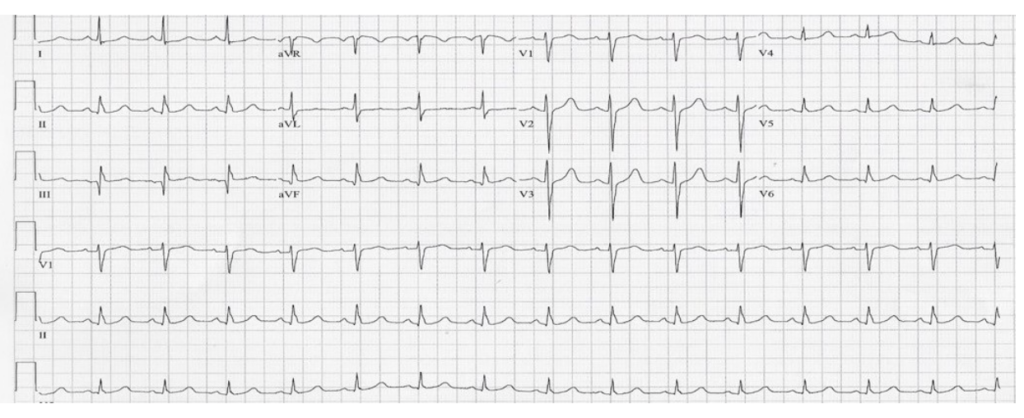
What was the 24-year-old female doing with the possible inferior MI, current or old?
She was taken to the hospital, and troponins were run, which were slightly elevated. Her glucose was elevated, and her history was revealed to the ER provider. She was on dialysis and she was insulin-dependent with a history of anemia of chronic disease, and hypertension.
Her diabetes and hypertension, that was undiagnosed and untreated led to her renal failure, which led to her dialysis, which led to her anemia of chronic disease.
Of course, because she had chest pain and slightly above-normal troponin she was admitted, and she had a stress test the next day. The stress test was very abnormal, so she was taken to the cardiac catheterization suite.
During her exam, her RCA and LAD were completely occluded 99% and two drug-eluting stents were deployed.
When she recounted the day, she said she didn’t feel well and felt a “little woozy.” The next thing she remembered was waking up when the paramedics arrived. The last thing she said was, “I’ve been telling the doctors for months that I’ve had chest pain, but no one will listen to me.”
This is another case of looking at the patient’s heart age, as opposed to their chronological age. The sign on her EKG that could have been a clue was her q wave in lead III that was pathologic.
Often young patients will be dismissed when they complain of chest pain. However, in her case, it was more important to recognize that her “heart age” was definitely older than 24. With her history of IDDM, CKD, anemia and HTN this elevated her risk.
So, when evaluating patients that are young with chest pain, make sure to do a thorough review of systems, history and family history. Have a strong index of suspicion, especially if somebody has a young family history of coronary artery disease.
With young patients although this case is rare, it is still possible and if we don’t cast a wide net, we can miss these cases.
Follow Jen on Social Media at Cardiology Made Easy
Skin Bones CME Conferences
Hit the reset button while earning continuing medical education credits at our CME conferences, where you can travel to a vacation destination; earn CME credits with like-minded nurse practitioners, physician assistants, and physicians; and ‘unplug’ while enjoying a new locale! Check out our upcoming Skin, Bones, Hearts & Private Parts 2023 CME Conferences and 2024 CME Conferences! At every event, the best of the medical community gathers to earn CME credits, network, and gain knowledge on dermatology, orthopedics, cardiology and emergency medicine, women’s health, pain management and pharmacology, diabetes, ER, and mental health. On-line CME courses and Virtual CME are also available so you have the option of earning CME credits online.